Ultrasound / White paper
Cardiac screening and profi ling of the elite academy footballer: How new heart imaging methods can help pick up underlying heart disease in young athletes
Nathan Ridinga,b, Craig Williamsc, Nuno Duarted, Diane Rydinge, A. Graham Stuartd,f, Eddie Craghille, Dave Perrye, Steve McNallye, Guido E. Pielesb,d,g
a. Bristol Medical School, University of Bristol, Bristol, UK
b. Institute of Sport Exercise and Health (ISEH), University College London, London, UK
c. Children’s Health and Exercise Research Centre, University of Exeter, Exeter, UK
d. Congenital Heart Unit, Bristol Royal Hospital for Children and Heart Institute, Bristol, UK
e. Manchester United Football Club, Football Medicine & Science Department, Manchester, UK
f. National Institute for Health Research Cardiovascular Biomedical Research Centre, Bristol Heart Institute, UK
g. Sports Medicine Department, Aspetar, Orthopaedic and Sports Medicine Hospital, Doha, Qatar

Introduction
The topic of sudden cardiac arrest is one that will strike a chord with football fans globally, with more attention than ever before being placed on these worrying events. The overall prevalence of sudden cardiac death in athletes is between 1:40,000 to 1:80,000 1. Some reports suggest that up to 65% of cases occur before the age of 17 2, with a large-scale study of English academy football players documenting an incidence as high as 1 in every 14,700 athletes3. While the reasons for sudden cardiac arrest are typically similar between adolescents and adults, there are differences in the commonality of certain conditions depending on age, largely due to maturation and the onset of diseases expressing themselves. Due to this and the fact that approximately 50-80% of cardiac arrests occur without warning4, cardiac screening was implemented as a means of trying to detect any underlying cardiovascular disease5, Indeed no fewer than 19 of the leading international sporting organizations, including FIFA, have recommended if not mandated its utilization in their athletes6.
We screen athletes specifi cally as among those with such underlying pathology, exercise may trigger fatal arrhythmias, resulting in a 2.8 to 5.3 times greater incidence of sudden cardiac death than their non-athletic peers7. The pursuit of success in the setting of professional football starts from as early as nine years old. In line with this, in the UK under the remit of the Elite Player Performance Plan, the volume of training provided to child athletes in the year 2012 was increased by 121%, up to a cumulative 8,500 hours in the academy period. Even by the age of 13, players are receiving between 10 and 12 hours of coaching per week. This volume of training lies within the parameters recently set by the European Society of Cardiology (ESC) as to defi ne an “elite” adult athlete8. This trend towards early specialization in soccer is placing increasing demands on the body, and we must be aware that the heart is a muscle and is adaptive and reactive to the loads placed upon it.
Due to these factors, cardiac screening to prevent sudden cardiac death is of high importance, and is recommended to start either at the onset of puberty or the start of competitive activity9,10. As detailed before, it means that in the setting of professional football it is not uncommon to initiate cardiac screening in the preadolescent years. The Football Association (FA) now recommends screening players several times throughout their career11. In this screening approach the proven diagnostic tools are medical history, examination, 12-lead electrocardiogram (ECG), often combined with a resting echocardiogram.
At Manchester United, to ensure both a comprehensive approach and to obtain novel research data to find the optimal approach to prevent sudden cardiac death and monitor the cardiac health of youth athletes, we have initiated a cardiac profiling program for academy football players who are screened every two years from the age of 12 (Figs. 1 and 2). Further, while current European and English FA guidelines recommend ECG and echocardiogram, it remains unknown if a more comprehensive approach can further improve results. In particular, heart imaging during exercise has entered the arena and with progress in imaging technology, hearts can now be evaluated during exercise at heart rates beyond 150 bpm, due to the quality of modern imaging equipment. Our research group is at the forefront in this area, and in collaboration with Canon has successfully developed a comprehensive approach to assess the cardiac health of elite academy athletes in a timely manner (Fig. 1). We are working on expanding this comprehensive cardiac profiling program into the relatively recently formed women’s squad, who at present receive cardiac evaluations from the age of 16 years onwards.
 Figure 1 State-of-the-art “one-stop-shop” cardiac profiling set up with resting ECG and echocardiography, followed by simultaneous exercise stress ECG, exercise echocardiography and exercise performance assessment using cardio-pulmonary exercise testing.
Figure 1 State-of-the-art “one-stop-shop” cardiac profiling set up with resting ECG and echocardiography, followed by simultaneous exercise stress ECG, exercise echocardiography and exercise performance assessment using cardio-pulmonary exercise testing.
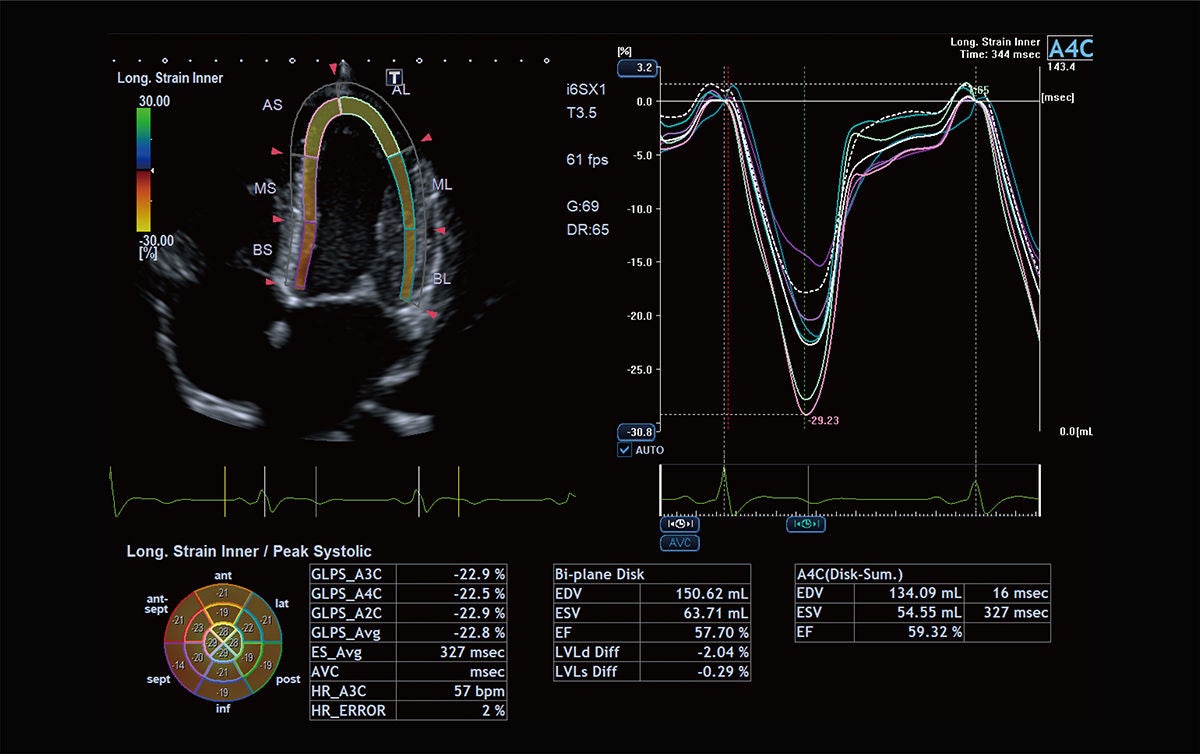 Figure 2 Left ventricular apical 4 chamber echocardiographic view. The Canon automatic wall motion tracking software allows the performance of 2-D strain analysis (myocardial performance at rest and during exercise).
Figure 2 Left ventricular apical 4 chamber echocardiographic view. The Canon automatic wall motion tracking software allows the performance of 2-D strain analysis (myocardial performance at rest and during exercise).
Medical history
Today there are numerous highly technical and advanced modalities to assess the cardiovascular health of our athletes, yet the history and physical remains the backbone of the screening process. It is advocated by all sporting and cardiology organizations including FIFA and the FA, and while several renditions of the questionnaire exist, they are all based on similar concepts regarding symptoms or a family history related to any genetic and congenital cardiovascular disease in which there has been shown to be an increased risk during exercise.
Concerns regarding the reliability of the screening questionnaire in children have been raised4, e.g., children with cardiac abnormalities may indeed have symptoms that may be dismissed or misinterpreted. Thus, the way the questionnaire is administered must be considered as the questions asked are highly dependent on interpretation of the athlete, and symptoms such as excessive fatigue or shortness of breath associated with exercise are often deemed the norm in the elite athlete. This may explain why initial rates of reported symptoms can be as high as 68%12 and sensitivity as low as 0%13-15. If the questions are not asked in a manner that is easy to understand, particularly when talking to children, and if no appropriate follow-up questions are asked to clarify the clinical significance of the answers, any false positive results may result in anxiety, unnecessary testing, delays and added cost. The role of an experienced physician is therefore paramount in obtaining a detailed past medical history, as 50% of positive athlete self-reported histories were deemed not clinically relevant for cardiac disease upon review16.
Physical examination
The second aspect to the consultation is the physical examination. Particularly in the pediatric athlete it is important to assess for the presence of congenital abnormalities and features associated with conditions such as Williams, Turner, or Marfan syndrome. In a meta-analysis comparing the effectiveness of all investigations however, the physical exam had the highest false positive rate, with murmurs and physical stigmata of Marfan syndrome being the most common cause. This questioning of the physical exam has been recently supported, with a recent study of over 5,000 children revealing that characterizing a murmur as physiological or pathological had no bearing on the presence of structural heart disease17. The American Heart Association (AHA) recommends the history and physical as the sole tool in athlete screening18, yet the consistently poor sensitivity and high false positive rate lends towards the potential role of other testing.
Electrocardiography
The next step of the profiling process is the ECG. While a review of all available research highlighted that the ability of the medical history and physical examination to accurately predict a diagnosis was just 20%, the ECG recorded a value of 94%1. Thus, the ECG is recommended by leading sporting organizations such as FIFA to be part of the screening process. The growth of ECG-led screening occurred following the results of a longitudinal Italian study, which showed an 89% reduction in sudden cardiac death rates following its implementation19. Despite these results, antagonists of ECG screening cite the cost effectiveness, need for experienced physicians and a high false positive rate as their reasons for excluding it20. There have however now been several iterations of the ECG interpretation criteria, which have decreased the false positive rate from 22% down to 5%21. There is no denying that should the false positive rate still remain at 1 in every five athletes, the process would need to be questioned. However today, it lies below levels seen in other commonly used screening tests such as those for breast or prostate cancer, simultaneously improving cost effectiveness22. These data however have been established for adult athletes and despite the previously mentioned figure of 70% of sudden cardiac deaths occurring in those under 17 years old, paradoxically there has been a shortfall in the literature regarding the ECG characteristics of the pediatric athlete and whether the same criteria apply.
A systematic review and meta-analysis from our group highlighted that pediatric athletes do indeed show a greater prevalence of ECG changes that are characteristic of high and continuous training levels than non-athletes, yet this was dependent on the age of the athlete23. It has only been in the most recent guidelines that any consideration at all had been placed on the age of the athlete, with the so called “juvenile” ECG pattern being considered normal in those under the age of 16 24. Using this classification in an analysis of academy football players, Malholtra and colleagues25 suggested that these guidelines are indeed applicable to adolescent athletes, however, they failed to account for the maturational status of the players. Using wrist X-rays to determine biological age, research from McClean and colleagues demonstrated its importance highlighting that by using this instead of the traditional chronological age, the diagnostic accuracy went from a “fail” to “excellent,” suggesting caution should be made if screening pediatric athletes without considering their maturational status26. This shows that despite strides forward in our interpretation of the athlete’s ECG, an understanding of the maturational development and highly variable rate of change in young athletes is imperative. This is needed together with a full comprehension of the key cardiac diseases which are more commonly identified in this younger age group, and how their presentation may be different to that of an adult. Our approach attempts to account for the changes due to growth and maturation by following the academy athlete over the years through puberty to pick up any suspicious changes.
Echocardiography
The cardiology bodies of the ESC9 and AHA18 do not endorse the use of echocardiograms in the screening protocol. Nevertheless a recent survey identified that only 8% of cardiologists never include it in the first line assessment of their athletes27. The reasons for not recommending it has been the publication of several studies which identified no athlete with significant pathology should they have already had a normal history, physical and ECG28-30. One sporting organization that do require it as part of the assessment of their athletes is FIFA31. Indeed it is in a study of adolescent football players where the value of echocardiography was shown3. Conditions picked up by echocardiography were arrhythmogenic cardiomyopathy, bicuspid aortic valve and two coronary artery anomalies. It shows that the test may enhance sensitivity, and this relatively inexpensive tool may reduce the number of days lost to sport in athletes that require further testing. The American College of Cardiology (ACC) “caution against its use outside of carefully controlled settings that are resourced with expertise in sports cardiology and the comprehensive non-invasive imaging resources required to evaluate positive or equivocal findings32.” With false positives, such as inconclusive identification of the coronary arteries, it highlights the need for experienced sports cardiologists and specialized equipment and infrastructure to be in place for echocardiography to be implemented. While in the setting of professional football in the UK, this is likely established, care must be taken if such a test is mandated, due to the global disparity in the finances and infrastructure of national football associations. The echocardiogram is in our opinion a key component of primary assessment but also further evaluations in the event of a positive downstream finding. The international ECG interpretation recommendations stipulate that 14 out of the 17 abnormalities should warrant follow-up with echocardiography33. Here, like the findings from the ECG, there is a grey zone between physiological and pathological adaptation and presents notable clinical dilemmas for the physician.
These conundrums are exacerbated when it comes to the echocardiographic evaluation of pediatric athletes34. Our recent meta-analysis highlighted that although pediatric athletes had similar cardiac function to non-athletes, their left ventricles were thicker and larger in diameter23. Nevertheless, normative data is often lacking within this group making it difficult to deduce what is normal from abnormal, especially as adult guidelines may not be appropriate. Work from our group is underway in identifying the normal limits of cardiac structure and function in the pediatric athlete. Using the advanced modalities of 2-D strain imaging (myocardial deformation imaging) it shows a promising role in the early differentiation of physiological versus pathological remodeling with our group already using the capabilities of the Canon systems in this area to publish reference values for adolescent athletes (Figs. 2-4)35. Echocardiography is therefore a primary profiling tool in our approach from the age of 14 years onwards, an age where we commonly observe the first presentation of the common inherited cardiomyopathies.
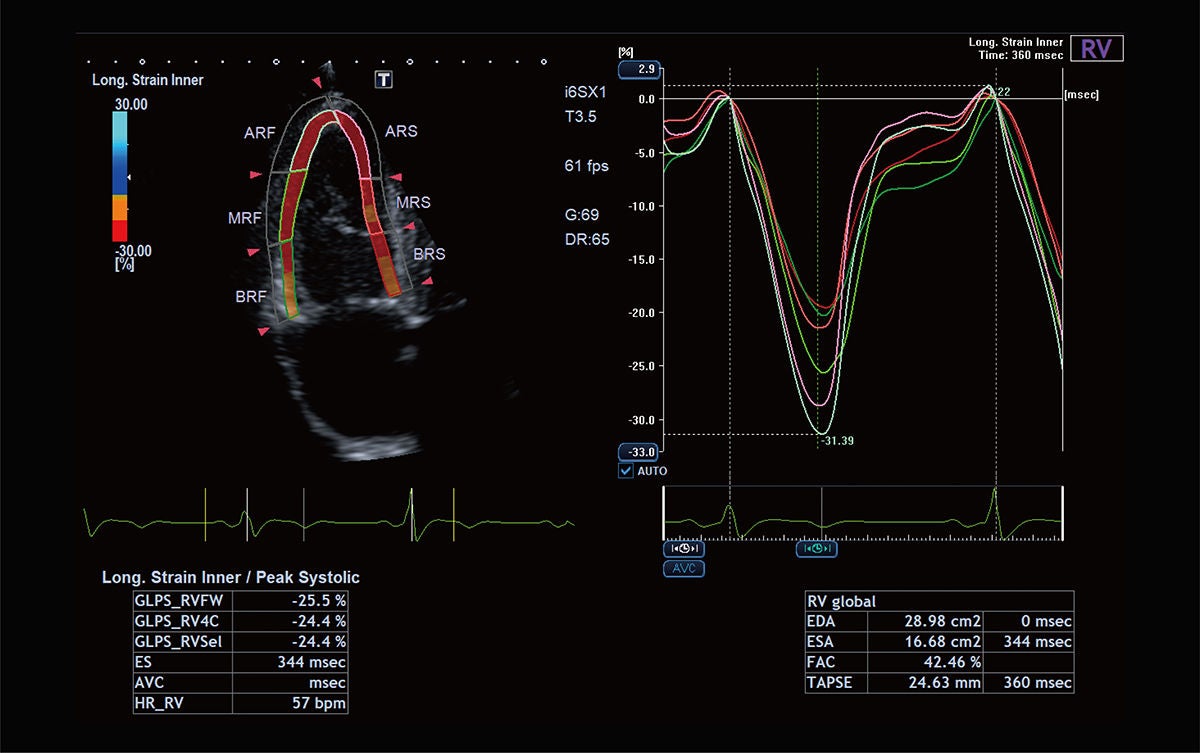 Figure 3 RV longitudinal 2-D strain analysis at rest and during exercise is important to exclude right-sided inherited pathologies such as arrhythmogenic cardiomyopathy.
Figure 3 RV longitudinal 2-D strain analysis at rest and during exercise is important to exclude right-sided inherited pathologies such as arrhythmogenic cardiomyopathy.
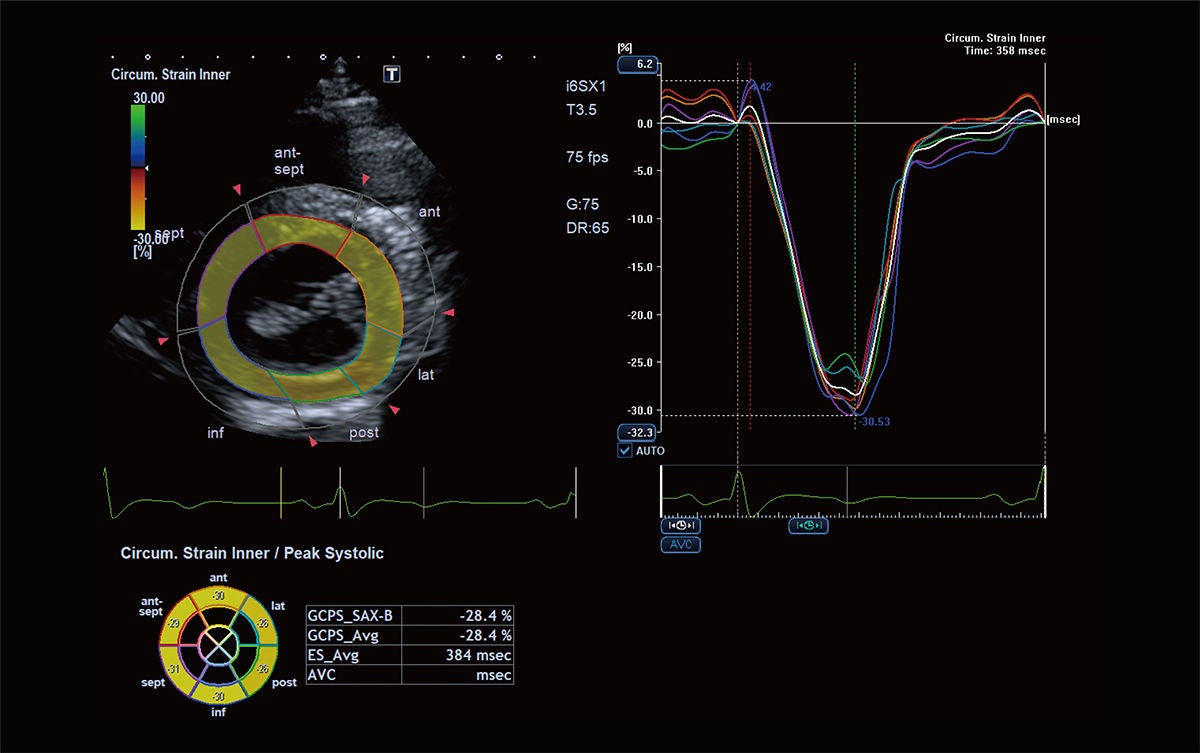 Figure 4 Left ventricular circumferential strain analysis has shown to be robust and predictive of exercise performance and should be used additionally to longitudinal strain during exercise; it can be used at basal, mid and apical levels (basal shown here).
Figure 4 Left ventricular circumferential strain analysis has shown to be robust and predictive of exercise performance and should be used additionally to longitudinal strain during exercise; it can be used at basal, mid and apical levels (basal shown here).
Exercise echocardiography
All examinations discussed so far have been based around an assessment of the heart at rest, the reason we screen athletes per se is however due to their increased levels of intense exercise. It may therefore seem pertinent to investigate the athlete’s cardiovascular system under these stressed conditions and this hypothesis lies at the core of our comprehensive cardiac profiling approach at Manchester United.
Similar to resting echocardiography, exercise echocardiography has not been recommended to be integrated into first-line screening practice. Improvements in imaging equipment, technology, and allowing the movement towards more robust quantitative analysis, has led this however to becoming more established in the secondary evaluation of cardiac abnormalities or disease. Within the pediatric congenital patient for example it allows us to assess their hemodynamic and myocardial responses. In such young patients, having an affordable, readily available, and non-radiating tool is invaluable in their long-term follow-up36. In the athletic population where, cardiac function may sometimes be lower than expected37, it allows us to classify whether it has a physiological or pathological origin, with advanced technologies such as strain being able to reveal signs of early cardiac dysfunction. This modality is again helping us decipher the grey zone of cardiac remodeling in athletes, and work from our group has gone some way to doing this within the pediatric footballer. Pieles and colleagues35 identified that the more reliable and valid measures of strain and strain rate during exercise were similar between the footballers and non-footballers. In highlighting the specific response to exercise this will allow us to help further differentiate between the adaptive, physiological response versus the maladaptive pathological myocardial function in pediatric athletes. Exercise echocardiography is in our approach complemented by simultaneous cardiopulmonary oxygen consumption (VO2) assessment, as it adds information on the metabolic and respiratory response to exercise. Besides the medical information it provides invaluable data on aerobic and anaerobic fitness for the sports scientist and coaching team. In our novel approach it provides for the first-time direct data on the much-investigated relationship between myocardial performance and metabolic parameters. A stress ECG run at the same time allows to exclude or diagnose exercise-induced arrhythmias, completing our cardiac profiling pathway.
Commonly, while state of the art, all these investigations can be time consuming, ECG, echocardiogram at rest, exercise echocardiogram and VO2 usually being spread out over several appointments in public but also private health care provision. Combining these investigations in a streamlined approach, we now routinely perform a comprehensive cardiac profiling assessment of an athlete within 75 minutes including a consultation with results and management plan if required (Fig. 5). Also of importance is that cross sectional imaging, such as cardiac magnetic resonance imaging (MRI) or computed tomography (CT) are available at the medical center at the Manchester United training ground (Fig. 6). Further accelerating time from initial cardiac profiling to diagnosis and ultimately return to play. Cardiac MRI specifically has recently become a mainstay secondary imaging method and is the gold standard for imaging of myocarditis and inherited cardiomyopathies. CT is useful to meticulously assess coronary artery morphology38, and availability at the assessment facility reduces the often stressful waiting time until exclusion or diagnosis, providing optimal player care and welfare. Additionally, the cardiac profiling set up described here provides a comprehensive research hub to further our knowledge in sports cardiology.
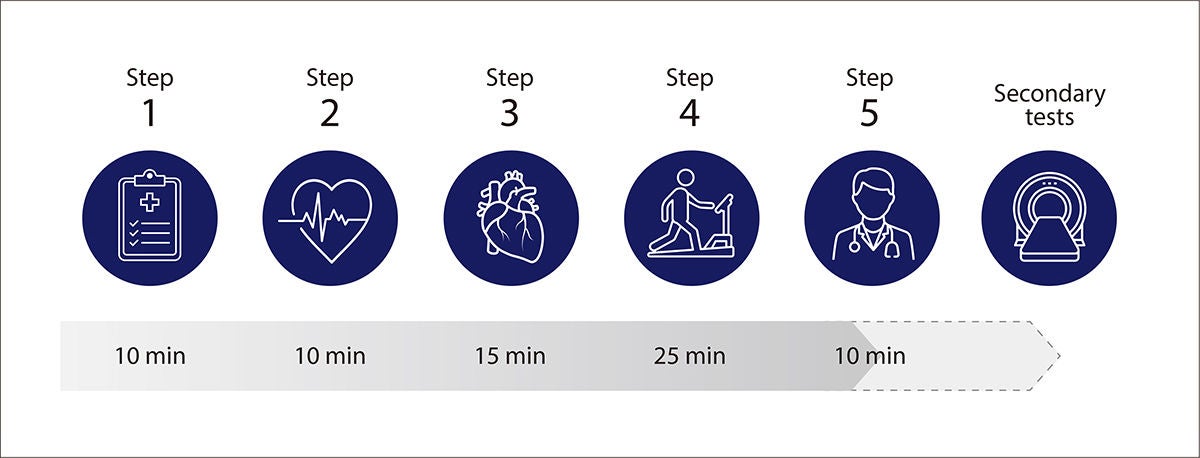 Figure 5 Flow of the “one-stop-shop” cardiac profiling approach. 1) History and physical examination 2) Resting 12-ECG 3) Resting echocardiogram 4) Simultaneous cardiopulmonary exercise test, exercise ECG and exercise echocardiogram 5) Consultation with Sports Cardiologist discussing results and outcome. This comprehensive approach, in the hands of an expert team, takes only approx. 70 minutes. Cardiac MRI and CT are also available at the profiling facility as secondary imaging tools if indicated.
Figure 5 Flow of the “one-stop-shop” cardiac profiling approach. 1) History and physical examination 2) Resting 12-ECG 3) Resting echocardiogram 4) Simultaneous cardiopulmonary exercise test, exercise ECG and exercise echocardiogram 5) Consultation with Sports Cardiologist discussing results and outcome. This comprehensive approach, in the hands of an expert team, takes only approx. 70 minutes. Cardiac MRI and CT are also available at the profiling facility as secondary imaging tools if indicated.
 Figure 6 CT (Aquilion ONE) and 3T MRI scanners (Vantage Galan 3T) as installed at the imaging suite at Manchester United. Cardiac MRI imaging in particular has recently become an invaluable secondary investigational tool to quantify cardiac function and volume and investigate for possible inherited cardiomyopathies and myocarditis. It is also gold standard in the assessment of cardiac fibrosis and inflammatory disease. MRI is often required as the final investigation to diagnose or rule out cardiac disease and allow return to play (RTP) and scanner availability at the training centre significantly reduces time to RTP.
Figure 6 CT (Aquilion ONE) and 3T MRI scanners (Vantage Galan 3T) as installed at the imaging suite at Manchester United. Cardiac MRI imaging in particular has recently become an invaluable secondary investigational tool to quantify cardiac function and volume and investigate for possible inherited cardiomyopathies and myocarditis. It is also gold standard in the assessment of cardiac fibrosis and inflammatory disease. MRI is often required as the final investigation to diagnose or rule out cardiac disease and allow return to play (RTP) and scanner availability at the training centre significantly reduces time to RTP.
Conclusion
Recent advances in ultrasound imaging technology are allowing us to better differentiate between what is a normal response to training and what is an expression of pathology. Given screening is often initiated in the pre-adolescent years, identifying these markers earlier through advanced methods such as myocardial wall motion tracking analyzing strain and strain rate is fundamental for the long-term care of our athletes. Exercise imaging, while not a primary screening tool, has its role in a more comprehensive cardiac profiling approach. Our pathway can easily be transferred to senior teams, and where clinically indicated, can be performed in a time-sensitive manner to deliver reliable cardiac results. Furthermore, research output from the collaboration of our research group, Manchester United and Canon Medical Systems has already resulted in introducing exercise echocardiography in the assessment of children with congenital heart disease in the UK National Health System (NHS) care pathway, thus contributing to improving not only the safe performance of the stars of tomorrow but also improving the health of children with heart disease.
References
- Harmon KG, Zigman M, Drezner JA. The effectiveness of screening history, physical exam, and ECG to detect potentially lethal cardiac disorders in athletes: a systematic review/meta-analysis. Journal of electrocardiology 2015;48(3):329-38.
- Maron BJ, Doerer JJ, Haas TS, et al. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980–2006. Circulation 2009;119(8):1085-92.
- Malhotra A, Dhutia H, Finocchiaro G, et al. Outcomes of Cardiac Screening in Adolescent Soccer Players. N Engl J Med 2018;379(6):524-34. doi: 10.1056/NEJMoa1714719 [published Online First: 2018/08/09]
- Drezner JA, Fudge J, Harmon KG, et al. Warning symptoms and family history in children and young adults with sudden cardiac arrest. The Journal of the American Board of Family Medicine 2012;25(4):408-15.
- Riding NRP, G. E. . Should cardiac screening be compulsory in athletes? Aspetar Journal: Aspire Publishing, 2019:4.
- Mont L, Pelliccia A, Sharma S, et al. Pre-participation cardiovascular evaluation for athletic participants to prevent sudden death: Position paper from the EHRA and the EACPR, branches of the ESC. Endorsed by APHRS, HRS, and SOLAECE. Eur J Prev Cardiol 2017;24(1):41-69. doi: 10.1177/2047487316676042 [published Online First: 2016/11/07]
- Drezner JA, Harmon KG. Incidence of sudden cardiac death in athletes. The ESC Textbook of Sports Cardiology 2019:299.
- Pelliccia A, Sharma S, Gati S, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease: The Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC). European heart journal 2021;42(1):17-96.
- Corrado D, Pelliccia A, Bjornstad HH, et al. Cardiovascular preparticipation screening of young competitive athletes for prevention of sudden death: proposal for a common European protocol. Consensus Statement of the Study Group of Sport Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J 2005;26(5):516-24. doi: 10.1093/ eurheartj/ehi108 [published Online First: 2005/02/04]
- Fritsch P, Ehringer-Schetitska D, Dalla Pozza R, et al. Cardiovascular pre-participation screening in young athletes: Recommendations of the Association of European Paediatric Cardiology. Cardiol Young 2017;27(9):1655-60. doi: 10.1017/S1047951117001305 [published Online First: 2017/08/10]
- Malholtra A, Sharma S. Lessons Learned From Mandatory Cardiac Screening of Young Athletes. Medscape 2018;09 November
- Fudge J, Harmon KG, Owens DS, et al. Cardiovascular screening in adolescents and young adults: a prospective study comparing the Preparticipation Physical Evaluation Monograph 4th Edition and ECG. British journal of sports medicine 2014;48(15):1172-78.
- Wilson MG, Basavarajaiah S, Whyte G, et al. Efficacy of personal symptom and family history questionnaires when screening for inherited cardiac pathologies: the role of electrocardiography. British journal of sports medicine 2008;42(3):207-11.
- Hevia AC, Fernбndez MM, Palacio JMA, et al. ECG as a part of the preparticipation screening programme: an old and still present international dilemma. British journal of sports medicine 2011;45(10):776-79.
- Fuller CM, McNULTY CM, Spring DA, et al. Prospective screening of 5,615 high school athletes for risk of sudden cardiac death. Medicine and Science in Sports and Exercise 1997;29(9):1131-38.
- Williams EA, Pelto HF, Toresdahl BG, et al. Performance of the American heart association (AHA) 14-Point evaluation versus electrocardiography for the cardiovascular screening of high school athletes: a prospective study. Journal of the American Heart Association 2019;8(14):e012235.
- Austin AV, Owens DS, Prutkin JM, et al. Do ‘pathologic’ cardiac murmurs in adolescents identify structural heart disease? An evaluation of 15 141 active adolescents for conditions that put them at risk of sudden cardiac death. British Journal of Sports Medicine 2022;56(2):88-94.
- Maron BJ, Friedman RA, Kligfi eld P, et al. Assessment of the 12-lead ECG as a screening test for detection of cardiovascular disease in healthy general populations of young people (12-25 Years of Age): a scientifi c statement from the American Heart Association and the American College of Cardiology. Circulation 2014;130(15):1303-34. doi: 10.1161/CIR.0000000000000025 [published Online First: 2014/09/17]
- Corrado D, Basso C, Pavei A, et al. Trends in sudden cardiovascular death in young competitive athletes after implementation of a preparticipation screening program. Jama 2006;296(13):1593-601.
- Sharma S, Estes III NM, Vetter VL, et al. Cardiac screening before participation in sports. N Engl J Med 2013;369(21):2049-53.
- Riding NR, Sheikh N, Adamuz C, et al. Comparison of three current sets of electrocardiographic interpretation criteria for use in screening athletes. Heart 2015;101(5):384-90.
- Asif IM, Prutkin JM. Modern standards of ECG interpretation in young athletes: Yield and eff ectiveness. Journal of electrocardiology 2015;48(3):292-97.
- McClean G, Riding NR, Ardern CL, et al. Electrical and structural adaptations of the paediatric athlete’s heart: a systematic review with meta-analysis. Br J Sports Med 2018;52(4):230. doi: 10.1136/ bjsports-2016-097052 [published Online First: 2017/04/02]
- Sharma S, Drezner JA, Baggish A, et al. International recommendations for electrocardiographic interpretation in athletes. European heart journal 2018;39(16):1466-80.
- Malhotra A, Dhutia H, Yeo TJ, et al. Accuracy of the 2017 international recommendations for clinicians who interpret adolescent athletes’ ECGs: a cohort study of 11 168 British white and black soccer players. Br J Sports Med 2020;54(12):739-45. doi: 10.1136/bjsports-2017-098528 [published Online First: 2019/07/07]
- McClean G, Riding NR, Pieles G, et al. Prevalence and signifi cance of T-wave inversion in Arab and Black paediatric athletes: Should anterior T-wave inversion interpretation be governed by biological or chronological age? Eur J Prev Cardiol 2019;26(6):641-52. doi: 10.1177/2047487318811956 [published Online First: 2018/11/15]
- D’Ascenzi F, Anselmi F, Mondillo S, et al. The use of cardiac imaging in the evaluation of athletes in the clinical practice: a survey by the sports cardiology and exercise section of the European association of preventive cardiology and University of Siena, in collaboration with the European association of cardiovascular imaging, the European heart rhythm association and the ESC Working group on myocardial and pericardial diseases. European journal of preventive cardiology 2021;28(10):1071-77.
- Riding NR, Sharma S, Salah O, et al. Systematic echocardiography is not effi cacious when screening an ethnically diverse cohort of athletes in West Asia. European journal of preventive cardiology 2015;22(2):263-70.
- Baggish AL, Hutter Jr AM, Wang F, et al. Cardiovascular screening in college athletes with and without electrocardiography: a cross-sectional study. Annals of internal medicine 2010;152(5):269-75.
- Magalski A, McCoy M, Zabel M, et al. Cardiovascular screening with electrocardiography and echocardiography in collegiate athletes. The American journal of medicine 2011;124(6):511-18.
- Thünenkötter T, Schmied C, Grimm K, et al. Precompetition cardiac assessment of football players participating in the 2006 FIFA World Cup Germany. Clinical Journal of Sport Medicine 2009;19(4):322-25.
- Baggish AL, Battle RW, Beaver TA, et al. Recommendations on the use of multimodality cardiovascular imaging in young adult competitive athletes: a report from the American Society of Echocardiography in Collaboration with the Society of Cardiovascular Computed Tomography and the Society for Cardiovascular Magnetic Resonance. Journal of the American Society of Echocardiography 2020;33(5):523-49.
- Drezner JA, Sharma S, Baggish A, et al. International criteria for electrocardiographic interpretation in athletes: Consensus statement. Br J Sports Med 2017;51(9):704-31. doi: 10.1136/bjsports-2016-097331 [published Online First: 2017/03/05]
- Pieles GE, Stuart AG. The adolescent athlete’s heart; A miniature adult or grown-up child? Clin Cardiol 2020;43(8):852-62. doi: 10.1002/clc.23417 [published Online First: 2020/07/10]
- Pieles GE, Gowing L, Ryding D, et al. Characterisation of LV myocardial exercise function by 2-D strain deformation imaging in elite adolescent footballers. European Journal of Applied Physiology 2021;121(1):239-50.
- Ermis P. Stress echocardiography: An overview for use in pediatric and congenital cardiology. Congenital Heart Disease 2017;12(5):624-26.
- Brown B, Somauroo J, Green DJ, et al. The complex phenotype of the athlete’s heart: Implications for preparticipation screening. Exercise and sport sciences reviews 2017;45(2):96-104.
- Pelliccia A, Caselli S, Sharma S, et al. European Association of Preventive Cardiology (EAPC) and European Association of Cardiovascular Imaging (EACVI) joint position statement: recommendations for the indication and interpretation of cardiovascular imaging in the evaluation of the athlete’s heart. European Heart Journal 2017;39(21):1949-69. doi: 10.1093/ eurheartj/ehx532
Learn more about us

Social Media


